



Breast Lift
Consultations offered at our three convenient locations in Encino, Glendale and Bakersfield
Time and gravity take their toll on your body, especially your breasts. Factors like pregnancy, weight loss, and aging cause the skin on your breasts to stretch, resulting in loss of elasticity. A breast lift, also called mastopexy, is a surgical procedure used to tighten the skin of your breasts and bring the nipples up. This procedure can also be combined with breast implants to enhance breast size at the same time. The result is the perky, firm breasts you enjoyed in your youth.
Although there are many products that promise a breast lift without surgery, mastopexy is still the best way to get perkier breasts that will last. Although your breasts will continue to age naturally following a breast lift, the results of your procedure should be long lasting. If needed, any breast asymmetry can also be corrected during your breast lift.
Contents
- 1 The Procedure
- 2 Before and After Photos
- 3 Breast Sagging – Ptosis
- 4 Surgical Techniques
- 5 Candidates
- 6 Preparations
- 7 Recovery
- 8 Q & A
- 8.1 Do I Still Need a Breast Lift if I get Implants?
- 8.2 Does a breast lift affect the look of the nipple-areola complex?
- 8.3 Does wearing a bra prevent breast ptosis or sagging?
- 8.4 Does breast feeding cause breast ptosis or sagging?
- 8.5 How Will Breast Lift Alter My Breast Size?
- 8.6 Does Mastopexy affect a woman’s ability to Breast Feed?
- 8.7 Mammogram and Breast Self-Examination
- 8.8 Can the areola size be reduced with a Mastopexy?
- 8.9 Can a Breast Lift Be Performed with Other Procedures?
- 8.10 What Is a Nipple Lift?
- 8.11 Breast Lift Without Implants
- 8.12 Is the Effect of A Breast Lift Permanent?
- 8.13 How long does a Mastopexy last?
- 8.14 How painful is a Mastopexy?
- 8.15 How soon can I expect to see the final result of a Mastopexy?
- 9 Risks & Complications
- 10 Concerns with Results
The Procedure

A Breast Lift, also known as Mastopexy, is a procedure to lift and reshape sagging breasts. According to the American Society of Plastic Surgeons, nearly 100,000 women underwent this procedure in 2005.
Any woman who has Ptosis, or sagging of the breasts, is a candidate for Breast Lift. Conditions that contribute to the Ptosis of the breasts include:
Aging: As women age, there is a gradual reduction in skin elasticity, as well as the stretching and elongation of the Cooper’s Ligaments, which are responsible for holding breast tissue up against the chest wall. The breast tissue itself also changes with age – from mostly firm, fibrous milk glands to fatty tissue, which is soft and saggy. This change accelerates with menopause, and the gradual reduction of estrogen levels.
Pregnancy and Nursing: Enlargement of the breasts during pregnancy, followed by their deflation after the end of breast feeding, also stretches the Cooper’s Ligaments, reducing fibrous tissue, breast volume and leading to Ptosis.
Large Breasts and Implants: The tissue and skin of inherently large breasts, or those that have been augmented with implants, stretch out from the breast weight, resulting in sagging.
Weight Loss: Rapid weight loss or dramatic fluctuations in body weight also cause the skin’s elasticity and breast tissue to decrease.
There are a variety of “litmus” tests to determine if the degree of sagging in your breasts is advanced enough to warrant a procedure. Many lay persons define breast sagging by how far the breast tissue descends on the chest wall. Plastic surgeons, however, define breast sagging based on the position of the nipple in relation to the breast mount – or Inframammary Fold. Degrees of sagging, each defined specifically by plastic surgeons are: Mild Ptosis, where the nipple is at the level of the Inframammary Fold; Moderate Ptosis, where the nipples have dropped below the level of the breast crease, but are still higher than that of most of the breast mount; Advanced Ptosis, where the nipples have dropped below the level of the Inframammary Fold and are just at the level of the maximum breast projection; and Severe Ptosis, where the nipples have dropped below the level of the Inframammary Fold, and below the breast mount, so they are pointing to the floor.
Breast augmentation after Pregnancy & Breastfeeding
Why many Los Angeles women seek to get breast implants after pregnancy? Breast feeding and hormonal changes of pregnancy diminish the breast volume and fullness. Loss of upper pole fullness and stretching of breast skin causes loss of breast cleavage and sagging. After pregnancy and breast-feeding women can no longer fill their tops and need push up bras and support to look like before. Breast implants with breast lift surgery enhance breast fullness and shape.
It is possible to augment the breast with fat grafting, but there are limitations on how much volume can be added to the breast, and the survival of the grafted fat.
There are many different breast implant sizes, shapes, and materials available, such as saline and silicone breast implants. The decision between saline and silicone implants requires considering many pros and cons of breast implant options, as well as the need to make breasts more even, and to lift breasts.
After pregnancy many women choose to have breast augmentation along with a tummy tuck which is called a Mommy Makeover.
#breastaugmentationafterpregnancy #breastimplants #afterpregnancy #breastimplants #salineimplants #siliconeimplants #mommymakeover #breastsurgery #beforeandafter #breastrecovery
Other “tests” for sagging include “The Pencil Test” that defines sagging breasts as those which hold a pencil in place under the breast under-fold. While many women consider some degree of sagging as normal and natural, The Bra Test determines that breasts which fall upon removal of the bra are Ptotic breasts.
Together, you and your plastic surgeon will determine which kind of Breast Lift procedure is best for you. During a Crescent Lift, the cosmetic surgeon removes a crescent-shaped piece of tissue above the areola and restores the tissue to a higher position. This creates a minor lift for patients who have Mild Ptosis. One risk of this technique is a slight egg-shaped areola for patients who have heavier breasts and do not wear good quality supportive bras following surgery.
Breast lifts achieve their final look by removing excess skin, tightening the surrounding tissue, and relocating the nipples to a higher position on the breasts. There are several ways this can be achieved; the best procedure for you will depend on a variety factors, including breast size and level of ptosis. Some procedures that Dr. Younai might recommend include:
Named for the crescent-shaped piece of tissue that is relocated during the procedure, this form of mastopexy is best for women suffering from mild ptosis. It can cause the areolas to develop an egg shape if the patient possesses heavier breasts or fails to wear the proper bra after surgery.
Also known as concentric mastopexy, this procedure involves the use of two concentric circular incisions around the areola to remove the tissue. It is ideal for women with smaller breasts and mild ptosis.
Similar to a Benelli lift, this variation makes straight incisions from the bottom of the areola to the fold beneath the breast. It is better for treating moderate ptosis.
Characterized by an anchor-shaped incision, a full breast lift is best for treating more extensive cases of ptosis.
No matter what your level of ptosis, there is a breast lift procedure that can help you. The surgery is generally performed on an outpatient basis under general anesthesia. During surgery, breast augmentation or breast reduction can also be performed. When combined with a breast lift, these procedures can help give better balance to your overall figure while creating a more youthful profile.
Before and After Photos



Breast Sagging – Ptosis

Although this question might seem moot, it is a question that I frequently get asked by women, because doctors and the general public define breast sagging and Ptosis differently. Some women think of their breasts as sagging if they have to wear a bra to hold them up! On the other hand, there are many women who feel that some degree of sagging is actually normal and natural. Unlike the public, the medical establishment defines breast sagging mostly based on the position of the nipple and its relationship to the breast mount. Instead, I find most women define sagging based not on the position of the nipples but on the extent of breast tissue descent on the chest wall.
Therefore, to answer the questions that “are my breasts sagging”, I recommend the following tests:
The Pencil Test
Place a pencil under the breast under-fold and if your breasts hold the pencil, then you have sagging.
The Bra Test

Do you need a bra to keep your breasts up on your chest? Do your breasts fall when you remove your bra? If your answer is yes, then your breasts sag.
Please note that these tests are not very reliable, because you can have breast tissue that is held up well, while the nipples are pointing to the floor! Therefore, the cosmetic surgeons define and classify the degree of breast Ptosis as follows:
Degrees of Breast Ptosis or Sagging
Ptosis is a sagging condition where the breast both falls on the chest, and points downward. Cosmetic surgeons determine the degree of Ptosis according to the position of the nipple relative to that of the inframammary fold – the fold under the breast. Officially, a young breast that is not sagging is defined as one where the nipple sits above the level of the Inframammary fold, where the bra wire goes.
The following are the degrees of ptosis that your cosmetic surgeon will considering in determining your need for a Breast Lift:
Grade I- Minor Ptosis
Nipple is at the level of the Inframammary fold.
Grade II- Moderate Ptosis
Nipples have dropped below the level of the breast crease, but still higher than the majority of the breast mount.
Grade III- Advanced Ptosis
Nipples have dropped below the level of the Inframammary fold, and just at the level of maximum breast projection.

Grade IV- Severe Ptosis
Nipples have dropped below the level of the Inframammary fold, and below the breast mount. They are pointing to the floor!
Pseudo-Ptosis or Glandular Ptosis
Nipple is at the normal level, but the breast Parenchyma has slid down below the level of the Inframammary fold, giving the appearance of a bottomed-out breast.
Surgical Techniques
There are several variations when it comes to breast lift surgery. The best procedure for you will depend on your level of sagging and the size of your breasts. All mastopexy procedures involve an incision near the areola, which is used to reposition the nipple higher up on the breast. One of the biggest concerns about breast sagging is the movement of the nipples, which point toward the floor in women with advanced sagging. Various incisions may be used to lift and tighten the breast tissue. Dr. Younai will assess your condition and go over your options during your consultation. Our goal is for you to be completely comfortable with every aspect of your procedure, especially the final results.

During Concentric Mastopexy, also known as the Benelli Lift, the plastic surgeon makes circular incisions around the areola, and removes the doughnut-shaped skin between the two incisions. The plastic surgeon then moves the nipple and areola upward and stitches surrounding skin around the areola. The Benelli Lift works best in women with smaller breasts and minimal sagging. A variation of this is the Benelli-Lollipop, which has straight incisions from beneath the areola to the mammary fold, rather than the circular ones. This is considered appropriate for women with Medium Ptosis.
Anchor-Shaped Mastopexy is the most common, and also the most invasive, Breast Lift procedure. Your cosmetic surgeon will make an incision above your nipple, in the shape of an anchor, with a circle at the top. The nipple is placed in the circle at the top of the “anchor,” forming the shape of the new breast. The lines at the bottom form the lower contour of your breast. The plastic surgeon sutures the skin around the areola, vertically down to the chest, and side to side along the newly created bottom fold.
Sometimes, Breast Lift is combined with a Breast Augmentation (with an implant) procedure to restore breasts to a fuller and enhanced appearance. At other times, Breast Lift is combined with Breast Reduction surgery, with the aim of lifting the breasts while reducing their size to a more proportionate one. One alternative to a Breast Lift is a Nipple Lift alone. While this will not raise the breast itself to the fullest extent possible, it has the advantage of leaving a scar only around the upper half of the areola.
Breast Lift/Mastopexy is a very technically challenging procedure that should be performed only by a board-certified plastic and reconstructive surgeon who is highly experienced in performing it.
Methods

All types of breast lift surgery ultimately have to satisfy two requirements. First, they have to match the surface area of the breast skin envelope to the volume of the breast, which is achieved by either removing excess skin and/or by increasing breast volume via addition of an implant. Second, they have to restore the nipple areolar complex’s normal location in relationship to the chest wall and breast mount. The following types of Mastopexy are designed to address different degrees of breast ptosis or sagging.
Crescent Lift for Minor Ptosis

The plastic surgeon removes a crescent-shaped piece of excess skin above the areola and repositions the nipple-areola complex superiorly by closing this gap. This results in a minor lift of up to one inch for patients who have minor ptosis.
Its advantage is that the scar is located at the periphery of the areola and thus is not noticeable. If needed, an implant can also be inserted through the same incision.
The disadvantages of this technique are that first, it can only achieve a minor lift, and second that by pulling the edge of the areola upwards there can be some temporary distortion of the shape of the areola depending on the degree of pull or lift.
Concentric, Peri-areolar, or Benelli Mastopexy for Moderate Ptosis
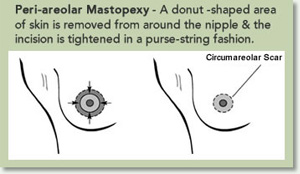
In this procedure, two circular or concentric incisions are made around the areola. A doughnut-shaped area of excess skin between the two incisions is then removed. By positioning the center of the outer ring of the doughnut higher than of the inner circle, the closure of this wound will result in superior repositioning of the areola-nipple complex.
The main advantage of this technique is that rather moderate amount of ptosis can be addressed without leaving a noticeable scar on the breast.
Its disadvantage is that it tends to stretch out and enlarge the diameter of the areola and flatten the nipple areola complex. Therefore, the breast loses its cone like projection. More importantly, this procedure carries a higher rate of recurrent ptosis as compared to the Inverted-T mastopexy. Women who have poor skin elasticity and more than mild to moderate ptosis can experience some recurrent sagging; usually requiring a second minor procedure where more excess skin is removed and the size of the areola is further reduced.
In terms of the scar appearance, although this scar is limited to the periphery of the areola, early on it may wrinkle or show some purse-stringing effect which usually resolves within weeks.
This technique works best for women with smaller breasts, and minor to moderate ptosis.
The Benelli-Lollipop Mastopexy

This technique is similar to the concentric lift, but with an extension of vertical scar extending to the mammary folds. It differs that the Inverted–T Mastopexy by eliminating the horizontal scar in the infra-mammary fold. This procedure is considered appropriate for those with medium ptosis that can’t be corrected with the Benelli Mastopexy, but who aren’t sagging enough to need a full Anchor or Inverted–T lift (see below).
Vertical Mastopexy- LeJour Mammoplasty
Madam LeJour, a plastic surgeon from Belgium, popularized Vertical Mastopexy in the 1980. This technique offered to lift the breast only with a vertical scar and without the additional horizontal scar, thus also being called a “short-Scar Mammoplasty.” In this technique the excess horizontal skin in the breast fold area is “bunched-up” into the vertical component of the scar. This “bunched-up” scar although being unsightly at first, would stretch out and flatten over several months after surgery. Because there is limit to how much skin could be gathered-up at the bottom of the breast, this technique is not ideal for women with large breasts or those with severe ptosis. Furthermore, I have found that in the today’s environment where women demand immediate results, many are not willing to wait five to twelve months until the unsightly gathered-up scar under the breast resolves.
Inverted-T or Anchor-Shaped Mastopexy
Inverted–T Mastopexy can achieve the tightest and most dramatic lift and is usually reserved for those with moderate to severe breast ptosis. It can eliminate excess breast skin, in both the vertical and horizontal dimensions. Because of this, it can create a breast that has excellent projection and a very “perky” look. It also carries a much lower incidence of recurrent ptosis as compared to the Benelli Peri-areolar Mastopexy.
This technique involves creating an opening in the shape of an anchor or inverted-T where the nipple is moved superiorly to the apex of the vertical incision and the base of the anchor is positioned in the Inframammary fold. Reshaping the breasts by this method involves extensive dissection of the breasts. This enables the surgeon to also remove excess breast volume from one breast in order to achieve size symmetry.

With respect to the resulting scar, the anchor or inverted-T scar tends to heal very well in the vertical limb. At times the horizontal limb of the scar can become hypertrophic and more noticeable, but fortunately this part of the scar is hidden in the Inframammary breast fold. Like Benelli Mastopexy, with this technique an implant can be inserted under the breast or chest muscle through the same incision. The combination of a breast lift and augmentation is called an Augmentopexy.
What Type Is Right For Me?
For women with moderate breast ptosis, the decision of which type of breast lift is a most difficult one, both the patient and the plastic surgeon. Obviously, everyone wants to have minimal scar, with the maximum breast projection, along with a natural looking breasts. Removal of excess skin results in a tighter breast but carries more scars. Sometimes, adding a breast implant to increase the volume of the breast relative to the breast skin envelope will help to reduce the excess skin to breast volume discrepancy, but note that placement of a larger implant will only help to some extent. Ultimately, the decision comes to choosing between a Benelli Peri-areolar Mastopexy and an Inverted–T Mastopexy. To make your decision you have to look more at the cons than the pros of each technique. If you absolutely object to having the more extensive Inverted–T scar and are willing to possibly undergo a second breast tightening revision, you might then consider a Benelli Peri-areolar Mastopexy. One the other hand, if you have to have the perkiest and most youthful breasts, and don’t mind having a bit more scars, then the Inverted–T Mastopexy is for you.
Candidates
Pregnancy. Nursing. Gravity. Loss of skin elasticity. All of these factors take their toll on a woman’s breasts over time. As this happens, your breasts often lose their shape. They are no longer firm. They sag.
No one has invented an antidote to gravity or to any of the factors that lead to drooping sagging breasts. No matter how hard you exercise or diet, it is not possible to rejuvenate your breasts to their original form or shape. Not even those creams or pills that are advertised over the internet help!
However, in the hands of a skilled plastic surgeon, you can raise and reshape sagging breasts through a Breast Lift, or “Mastopexy” and regain your more youthful figure.
No one can turn back the clock. However, a skilled cosmetic surgeon can indeed help you to regain your perky breast shape and form of your youth. The inevitable toll of pregnancy, gravity and the sagging that occurs with aging can be addressed through a Breast Lift. Especially for women who have started to doubt their femininity and sexuality, a Breast Lift can be a very helpful procedure.
A Breast Lift, also known as “Mastopexy” is a procedure to lift and reshape sagging breasts. Sometimes, it is combined with a Breast Augmentation procedure to restore breasts to a fuller and enhanced appearance, in which case it is called an Augmentopexy. Other times it is part of a breast reduction surgery, with the aim of lifting the breast while reducing their size to a more proportionate one.
The removal of excess skin with the rearrangement and re-suturing of breast tissues literally lifts the breast. Almost 100,000 women annually undergo this procedure. The American Society of Plastic Surgeons reported that 92,740 Breast Lifts were performed in the United States in 2005.
Reasons For A Breast Lift
“With time and childbirth, my breasts were never the same. I didn’t want to feel bad about how they sagged and drooped anymore. After interviewing several cosmetic surgeons, I opted for a Breast Lift, combined with having implants put in. This has restored my fuller, sexier look.” — Lucy, age 39
Any woman who has sagging or Ptotic breasts is a candidate for a breast lift or Mastopexy. There are several conditions or lift events that contribute to the sagging of the breasts:
Aging
As women age there is a gradual reduction in the skin elasticity, as well as the stretching and elongation of the Cooper’s Ligaments, which are responsible for holding up the breast tissue against the chest wall. The breast tissue itself also goes through changes with age. The breast substance or “Parenchyma” changes from one of mostly milk glands which are fibrous and firm to fatty tissue which is soft and saggy. This becomes accelerated with menopause and gradual reduction of estrogen levels. Therefore, one of the benefits of estrogen supplements in post-menopausal women, is having firmer and more youthful breasts.
Pregnancy and Nursing

Along with age and gravity, pregnancy and nursing take their toll on breast firmness and volume. Enlargement of breasts with pregnancy followed by their deflation after end of breast feeding results in stretching of the Cooper’s Ligaments as well as loss of breast Parenchyma and volume. The combination of the loss of supportive ligaments as well as loss of volume results in the Ptosis or sagging of breasts.
Weight Loss
Rapid weight loss or frequent dramatic fluctuations in body weight leaves its toll on the breasts. One of its signs is the appearance of stretch marks on the breasts which signify the loss of skin elasticity and breast tissue. With the increasing prevalence of Gastric bypass Bariatric Surgery more women are now facing Breast Ptosis, after having gone through post-surgical massive weight loss.
Large Breasts & Implants
The larger the breast weight, either by having inherently large breasts or by getting very large breast implants can stretch out the breast tissue and skin, resulting in breast sagging and Ptosis.
Post Mastectomy Reconstruction

Women who have had breast reconstruction after mastectomy, often times have their other breast lifted, so that it would better match their newly reconstructed breast.
Implant Removal
Removal of a breast implant leaves the breasts sagging due to excess skin. This can be corrected with a Mastopexy.
Preparations
The surgeon will provide very specific instructions prior to surgery so you will have an optimal and safe experience. These include what medications to avoid to prevent excessive bleeding and bruising, required medical exams, what to eat and drink prior to surgery, and the prescription of an anti-nausea pill to take on the morning of the surgery.
In all cases, you will be asked to have a reliable friend or family member take you home after the surgery, as you will not be allowed to drive.
- Tend to all of your chores and to do things before your surgery so you don’t have to worry about taking care of things early during your recuperation. You are not allowed to engage in heavy lifting for several weeks after surgery. This means if you usually clean the house, you should do so in advance of your surgery.
- Have your hair cut and colored, wax your legs, pay your bills, and take your dog to the vet before your planned day of surgery!
- If you an avid tanner, don’t tan your breasts for one week before, and six weeks after, your surgery. Any sun or tan burn of your breast skin can potentially increase the risk of infection of skin damage with breast augmentation.
- If you have nipple rings you must replace them with a plastic ring at least one week before surgery and wait for your surgeon to tell you when you can have them replaced.
- Rent your favorite movies and leave easily prepared foods and snacks in areas where you will not have to lift or reach.
- Place all of the medications, tissues, reading materials, water bottles on one table, within easy reach.
- Have ready ice cold cola drinks, ginger ale, or sport drinks close to your bed. Avoid drinking too much plain water after surgery, because it makes you more nauseated.
- After surgery take your nausea pill about one hour before your other medications to lessen nausea. Also, have some over-the-counter anti-acids available at your bedside.
- Some surgeons recommend putting cold packs on you breasts afterwards. In my opinion, even though cold might lessen the inflammation, it can also cause frost bites or skin damage while your breasts are numb after surgery.
- Pain Pump is a relatively new device used to deliver anesthetic solution into the breast tissue during the first 48 hours after surgery. It is the size of a walkman radio that is connected to breast via two very thin catheters that deliver the anesthetic solution. This machine reduces but does not eliminate the need for taking oral narcotics. Patients that are very sensitive to pain or cannot tolerate oral narcotics find this device very useful. Others feel that it is cumbersome especially that it is attached to your breasts for two days.
- Arnica Montana or Bromelain homeopathic herbs have been used in Europe for centuries to treat swelling, soreness and bruising. When properly prepared, Arnica may significantly decrease the healing time or the appearance of such. There are many formulations from different companies. Sublingual (under the tongue) types are the most often recommended for plastic surgery. I have seen variable results with its use. There are some patients that did not benefit from it and other who appeared to benefit. Therefore, I am open to its use if a patient would like to use it.
Qualified Surgeons
You would not select a Beverly Hills dentist to perform a Face Lift. Similarly, you should not jeopardize the outcome of your Breast Lift Surgery, or your well being, by choosing anyone less than the most qualified Board-Certified plastic surgeon.
While many states allow any licensed doctors such as a gynecologist, general surgeon, or otolaryngologist to perform cosmetic surgery, that does not mean that these physicians have
had the extensive formal training in cosmetic surgery that is taught to a Board-Certified Plastic Surgeon. In some states, even dentists are lobbying to perform cosmetic procedures.
Breast lift surgery or Mastopexy is a very technically challenging procedure you should only trust a board-certified plastic and reconstructive surgeon who have had experience in it. You should also choose a plastic surgeon who will show you solid “Before and After” examples of his or her work, and whose artistic sense is in sync with the results that you are seeking.
In choosing a surgeon to perform Breast Surgery, you should first choose one who has been certified by the American Board of Plastic Surgery (ABPS): (www.abplsurg.org).
This assures that the plastic surgeon has endured the most rigorous training possible, including three to five years of training in general surgery and two years of training in plastic surgery. Beware of those physicians who claim to be “board-certified” cosmetic surgeons. This may mean that they have taken a brief weekend course in a procedure but does not guarantee the competence that the American Board of Plastic Surgery ensures. Ideally, you will choose a surgeon who has extensive Breast Surgery experience, not only experience in plastic surgery in general. Breast Surgery, like sculpturing, is an art that is learned through experience, but can only be perfected by the plastic surgeon who has an eye and feel for body proportions and contour. This ultimate expert should be an artist as well as a skilled surgeon.
Pre-Operative Checklist
- If you are older than 45 years, or have heart disease, we require a pre-operative EKG, which would either be done by your internist, cardiologist, or at our facility. Heart disease and all other medical illnesses need to be optimized by, and you be cleared by an internist or specialist prior to surgery.
- Pre-operative laboratory blood and urine tests are done usually within 10 days of your surgery date. If you do have health insurance this might be covered, otherwise, the laboratory will charge you.
- If you have specific medical illnesses, allergies, or physical handicaps, please notify our staff during your pre-operative visit.
- Please refrain from taking any Aspirin, Aleve, Advil, Motrin or other NSAID for ten days prior to your surgery. These drugs can increase the incidence of bleeding and bruising.
- Do not drink or eat after midnight on the night before your surgery. This means no coffee or breakfast in the morning of your surgery. You should take all of your medications with a little water.
- Please remove and leave behind all jewelry, watches, and body rings before you come in for your surgery. Please do not wear any makeup, body lotion, or perfume.
- Before leaving home for your surgery, take one “nausea pill” — COMPAZINE — with a little water.
- Please wear comfortable and loose clothing the day of surgery. It would be helpful if you wear front open tops and loose sweatpants.
- If you have long hair wear a non-metallic cloth ponytail.
- Do not wear very dark nail polish.
- You should make arrangements for a friend or family member to take you home after surgery. You are not allowed to drive yourself home or take a taxi.
Recovery
The results of your breast lift will be the youthful, perky breasts you had when you were younger. The tissue will be elevated and the nipples will once again face forward. The final shape should be similar to wearing a supportive bra, even without support garments. If you choose to combine your breast lift with breast augmentation, you can also look forward to increased size. Dr. Younai will be on hand throughout the recovery process to ensure the best possible outcome. He can answer any questions you may have and will proactively check with you to make sure everything is going smoothly.
Dos and Don’ts!

Mastopexy generally takes between two to four hours, as an outpatient surgery. Afterwards, you will spend some time in the Recovery Room of the surgical facility. When you wake up, you will have gauze dressing over your breasts, and a support bra.
Your cosmetic surgeon will provide you with specific instructions for your recovery, including what medications to take and how to limit your activities.
- After surgery the best comfortable position for the first 2-3 days is to be lying semi-reclined. Elevation of the upper body and chest reduces the swelling and aching of the breasts.
- After one week you can sleep on your sides, and after two weeks, on your abdomen.
- I encourage you to be mobile and not to be sedentary in order to reduce the chance of forming blood clots in your legs.
- Some women develop back pain or muscle spasm as a result of sleeping propped up. If you experience this put a heating pack on your back and have your family member massage your back.
- Take your nausea medications about one hour before taking your antibiotics and pain medication in order to lessen the extent of nausea.
- It is good to stay well hydrated but avoid drinking too much plain water because it can make you more nauseated.
- Avoid eating greasy or spicy foods for the first three days and have anti-acids available if you get an upset stomach.
- Your gauze dressings will be removed in two days and afterwards you will be able to take a shower and get your breasts wet. After showering, you should blow dry the steristrip paper tapes that cover your incisions so that they don’t come loose. You will be keeping them on for about three weeks.
- Apply heavy lotion to your breast and abdominal skin away from your wounds to lessen the skin dryness that follows surgery.
- Recovery varies for each patient, as will the timing for resuming exercise and normal physical activities. Although you will probably be able to return to work within one to two weeks, your cosmetic surgeon will instruct you to avoid heavy physical exertion, including heavy lifting, frequent bending, reaching high over shoulder, and jogging for the first three to five weeks.
- Do not wear underwire bras or sport bras for the first several weeks because they tend to cut into your incisions (Inverted-T Mastopexy) and may push your breasts to set in a location too high. Your surgeon will tell you when you can get these bras. The best type of bra to wear during this period is a “sleep-in” bra. If you can’t find them, just get soft bras, and remove the under-wire.
- Be aware that your menstrual cycle may be altered for a month or two but should return to normal.
- You cannot get nipple or breast piercing, tattoos, or tan for at least six weeks after your surgery.
- You can have sex after one week, as long as you don’t overly exert yourself, and keep your incision clean and dry for up to 3-4 weeks.
- Be aware of doors when opening them. Often times, I hear women complain that after surgery they accidentally hit their breasts against them because they were not aware of the change in their body shape.
- You can not use a public pool, Jacuzzi, or go into the ocean for at least 4 weeks after surgery.
Post-Operative Instructions

- You will have some pain and nausea after your surgery. Your physician will prescribe the appropriate antibiotics and pain medications.
- For the first two to three days, sleep with your head elevated.
- Do not sleep on your stomach or sides until cleared by your physician.
- Do not remove your bandages until instructed to do so by your physician.
- Do not drink alcohol, take aspirin, or diet pills until your physician gives you approval to do so.
- Refrain from smoking for at least two weeks.
- Wear soft bras or maternity bras with NO under wire for at least six months after your surgery.
- You may walk, but you cannot participate in sports or strenuous physical activities until cleared by your physician.
- Do not raise your arms above your head for two weeks. This can potentially cause a displacement of your implants.
- Areas of your breasts or nipples will be numb for several weeks after surgery. This is normal and expected.
- The day of your surgery, wear loose, comfortable clothing that opens in the front, such as a jogging suit. Wear shirts that button down the front, and don’t need to be put over your head.
- If you have any important or urgent questions within the first week after surgery, you are welcome to call our office at any time.
Expectations

When you awake from surgery, you will have an elastic bandage or a surgical bra over gauze dressings. You should make an effort to move the day after your surgery, even if you don’t feel like it. It is good for your circulation and for your healing.
You should avoid lifting, bending and straining in any way. Also, be sure and sleep on your back, rather than on your stomach, to avoid placing pressure on your breasts.
Do not be alarmed if you feel discomfort from bruising and swelling. This is a normal result of the surgery, particularly for the first 48 hours. Your cosmetic surgeon will prescribe medications to relieve this discomfort.
At your first office visit following surgery, the bandages or surgical bra will be replaced with a softer support bra, which you will wear all of the time, day and night, for three to four weeks. These will help your breasts to retain their new shape.
There would be no sutures to be removed. The Steristrips that are applied to your incisions will either fall off in about three week or you can gently remove them by then.
Tips For Significant Others
The support of your family and loved ones can be as important to your healing as following your physician’s medical directives. Their understanding of the pain, discomfort, and at times, the roller coaster of emotions, that you might experience can make all the difference in having an optimal outcome.

- You should be available as a full time caregiver for at least 48 hours to help the patients with the tasks that are normally taken for granted, like being able to walk to the bathroom.
- You, or someone, should care for the patient’s children for a minimum of two to four days, and be sure that she has assistance in lifting young children for several days after your surgery.
- Help with pet care. Someone should walk them, feed them and clean up after them for at least several days.
- Prepare to help the patient address the swelling that she will experience, according to her physician’s instructions. This may include ice packs or gel pack specifically designed for breast surgery patients.
- Know that she may experience mood swings, and feel like crying off and on – especially in the first couple of weeks. This is a normal aftermath of major surgery.
- Encourage her to drink lots of water – to address bloating and to keep her hydrated.
- Remind her to not fight the pain – she should go with the flow, and take her medications as directed. It is not good to try and be a hero!
- Have her use a U-shaped pillow for sleeping and resting.
- Give her lots of compliments. She may be fearful because it will take some time before her new breasts appear as they should. She has a lot of healing to do!
- Prepare simple and easily digestible foods, such as scrambled eggs or Jell-O.
- Remind her to sleep on her back!
- Have two sleep-in bras at the ready – one tight and one loose to alternate as needed.
- Be there when she goes to have her bandages removed, to support her through any discomfort she may be feeling.
- As far as sex is concerned, let her initiate things and play it by ear.
- Some women are fearful that they might harm their implants if they are touched or manipulated after surgery. Have them ask their doctor about this and get some reassurance.
- Some women feel depressed or regretful about having undergone breast surgery. Sometimes they don’t know how to handle the attention or questions that breast surgery will bring about. At the same time, significant others can develop uneasy feeling about the fact that you underwent such surgery. It is good to talk about your feelings and to even seek outside help if you can’t resolve some ambiguities
Q & A
Do I Still Need a Breast Lift if I get Implants?
Breast implants replenish the lost volume of a sagging breast. Although implants fill the breasts, they result in only a very minimal lift if any, depending on the extent of skin laxity. Therefore, the premise that by choosing a bigger breast implant you can avoid the need for a breast lift is false.
Does a breast lift affect the look of the nipple-areola complex?
As the breasts sag the nipple-areola complex also stretches and gets larger. It is customary to reduce the size of the areola during a breast lift or Mastopexy procedure to that of a normal sized areola which has a diameter of approximately 1.5 inches.
Does wearing a bra prevent breast ptosis or sagging?
Although the sagging of breasts depends on a multitude of factors that were discussed earlier, in women with large and heavy breasts bra support will prevent excessive stretching of the Cooper’s Ligaments, thus diminishing the extend of sagging.
Does breast feeding cause breast ptosis or sagging?
Breast feeding by itself does not cause ptosis, but the enlargement of the breasts followed by the drying of the milk causes stretching of the breasts which can cause them to sag.
How Will Breast Lift Alter My Breast Size?

As a rule, a Breast Lift will reduce the size of your breasts – generally by one cup size. This is due to the removal of excess breast skin, which itself carries a certain volume. To compensate for the lost breast volume, you may then consider having an implant placed along with your Breast Lift. There are many factors to consider, such as your original breast size, what you consider most attractive, and your surgeon’s assessment of what size breasts are most proportionate for your body.
Does Mastopexy affect a woman’s ability to Breast Feed?
Considering that most types of breast lift or Mastopexy do not disconnect the nipple from its roots, a woman should be able to maintain her breast feeding ability after a lift. Nevertheless, a Mastopexy can alter a woman’s breast feeding ability if the surgery requires cutting into or manipulating the tissue located directly under the nipple-areola complex.
Mammogram and Breast Self-Examination

Mastopexy does neither alter your ability for breast self-examination, nor is it a hindrance for receiving a mammogram. Most surgeons recommend that you get a mammogram six months after your Mastopexy in order to establish a baseline.
Can the areola size be reduced with a Mastopexy?
Yes. The diameter and size of a stretched-out areola can be reduced via a Peri-areolar or an inverted–T mastopexy.
Can a Breast Lift Be Performed with Other Procedures?
Yes. Often, your cosmetic surgeon will determine that the optimal effect will be achieved when the lift is combined with the placement of a breast implant — Augmentopexy. This combination will give you the lift and the fullness needed for a more proportional figure.
Mastopexy can be combined with other procedures, as well. It is not uncommon for women who had breast implants at an early age, and now need to have their breast lifted, want to change the size or type of their breast implant to better fit their current figure and lifestyle. In this situation a breast implant exchange can be performed simultaneously with a breast lift. Some plastic surgeons recommend performing these two procedures at a separate time, but I find that you can get better overall results and less exposure to general anesthesia when both procedures are combines.
There are some women who have developed Capsular Contracture or tight scarring around their implants which makes their implants hard and painful. When performing a Capsulectomy in order to remove the hard capsule it is sometime necessary to further shape and lift the breast, thus requiring a Mastopexy at the same setting.
Finally, there are women who have had gained and lost much weight with their pregnancy, resulting in sagging breasts and abdominal folds. These women often opt to undergo a tummy tuck or abdominoplasty at the same time of a mastopexy or Augmentopexy.
What Is a Nipple Lift?

A Nipple lift is nothing other than a crescent mastopexy. In this procedure a crescent shaped section of excess breast Skin is removed above the areola. The nipple-areolar complex is then pulled upward to a new position and sutured into place. One disadvantage of this procedure is that the areola may become somewhat elongated.
Breast Lift Without Implants
As discussed earlier a breast lift or mastopexy can be performed without having to also have breast implants. But you have to be aware that a breast lift reduces the size of the breast by about a cup size. If your breasts are just a little too big, then a breast lift will also reduce their volume to an ideal size. On the other hand, if your breasts are currently just a little too small, a Mastopexy will make them even smaller. You might then consider having an Augmentopexy, instead.
Is the Effect of A Breast Lift Permanent?
As with any other body part, gravity, pregnancy and aging take their effect, even on Breasts that have been lifted. In some cases, women may opt for another procedure some years hence. A Breast Lift combined with an implant is generally longer lasting.
How long does a Mastopexy last?
Any surgery cannot be considered permanent as far as gravity goes. Gravity will prevail and you will sag, period. Although we can attempt to slow its process by wearing bras, staying out of the sun and healthy eating. Whatever the case, a woman’s breast tissue, in 95% of cases, will sag eventually. Regardless of having had Mastopexy, a breast will sag again. It may be years from now, but you may need an additional Mastopexy, depending on your habits of bra wearing, this may be slower. The type of a breast lift also affects the longevity of your lift. Usually, an Inverted–T Mastopexy will have a more lasting result than a Benelli Peri-areolar Mastopexy. The size and weight of your breasts also affect the natural progression of sagging. The heavier your breasts are, or the larger the implants, the faster your breasts can sag, if you don’t wear adequate breast support. Finally, the elasticity of your skin and breast tissue impacts the rate of their sagging. Women who have thin and sun damaged breast skin with many stretch marks have very poor skin and breast elasticity and will need a revision breast lift sooner.

It is supposed that after an Inverted–T Mastopexy a breast may start to sag again after 5-7 years with part time bra wearing, less than half that if a bra is hardly worn. If you have very thin skin, it takes even less time. Be safe and wear a bra.
How painful is a Mastopexy?
A Mastopexy is usually not as painful as a sub-pectoral breast augmentation, because it does not involves manipulating or stretching the muscles. It is also not as painful as a tummy tuck, or hysterectomy, but is more painful than having undergone a tubal ligation, appendectomy, or cholecystectomy (gallbladder removal).
Most women say that the worst of the discomfort is during the first two to three days. The prescribed pain medication makes this discomfort tolerable during this period.
How soon can I expect to see the final result of a Mastopexy?
The final result of a Mastopexy becomes apparent with your breast skin stretches and the breast mass settles into its final position. While with a crescent lift you can reach the final result by about six weeks, with a peri-areolar or more so an Inverted–T mastopexy this process takes several months. There are even times when an adjunct procedure or revision is planned during this period which will further delay the final outcome. Therefore, you need to be patient.
Also note that if you are having an Augmentopexy when an implant is inserted, the settling of the implant does also affect the shape of your breasts and the duration of your progress.
Risks & Complications
As with any major surgery, your risks are higher if you have diabetes, poor circulation, heart, lung or liver disease, if you are a smoker or have a family history of blood clots. Your cosmetic surgeon will want to assure that any medical conditions have been treated, and optimized, before you can consider having a Breast Lift.
Infection
The risk of wound infection is less than two percent. Most patients receive intravenous antibiotics during surgery and antibiotic medication after surgery, which minimizes this risk. Sometimes accumulated of blood (hematoma or seroma) can become infected, requiring drainage and further coarse of antibiotics. In extremely rare instances, life-threatening infections, including toxic shock syndrome have been noted after breast surgery. Individuals with an active infection in their body or weakened immune system should not undergo breast surgery.
Bleeding
While this is unusual, it is possible to experience a bleeding episode following surgery. If this occurs, emergency treatment to drain accumulated blood, or a blood transfusion, may be required. You can reduce this risk by not taking any aspirin or anti-inflammatory medications for ten days before or after surgery. Non-prescription “herbs” and dietary supplements can also increase the risk of bleeding. The risk of major bleeding, or blood collection, is only about three percent. Most women lose about two test tubes of blood during surgery. Any blood clots that form must be removed in a later surgical procedure.
Hematoma & Seroma
Sometimes blood in the depth of the breast tissue can accumulate and form a blood collection, called a Hematoma. Seroma is a fluid that arises from the breakdown of accumulated blood or Hematoma. In cases with extensive dissection and manipulation of the breast tissues, most plastic surgeons place a drain in the depth of the breasts to remove accumulated blood and fluid and thus prevent formation of a seroma. After drains are removed, this fluid may re-accumulate in the breasts, especially following trauma or vigorous exercise. Additional treatment may be necessary to drain the accumulation of fluid from the breast.
Pain
As is the case with any major surgery, a Breast Lift involves pain. Most women say that the pain is greatest in the first 48 hours after surgery. However, this will be minimized by the prescription that your cosmetic surgeon will prescribe before you go home. In very rare cases there are some women that develop chronic or long-term pain that will require further treatment.
Scarring
All surgeries of the breast involve some scarring, which is permanent but will fade with time. People scar differently, and some women are more delicate than others. All scars appear red and lumpy at first. Also, some ethnic groups are prone to the formation of thicker scars. Your pattern of scarring in the past could be a good predictor of how you will scar following a Breast Lift. In most women, the scars will be less noticeable within one year. In rare cases, scars may require surgical revision or treatment. Poor healing and scarring are more common in smokers.
As a rule, your cosmetic surgeon will place incisions in areas that can be covered by a bathing suit or under garments.
Change in Nipple and Skin Sensation
After breast surgery, it is normal to experience temporary numbness of the skin and the nipples. This usually resolves from six weeks to six months. During this period, you may even experience a period of increased sensation or hypersensitivity that can be treated with massage. Permanent partial or complete loss of nipple and skin sensation can occur following a Breast Lift in one or both nipples. This can depend on the extent of breast surgery. However, since the plastic surgeon doesn’t detach or remove breast tissue, nipple sensation is usually preserved. In general, the incidences of partial or complete loss of nipple sensation are each about 10%.
Asymmetry
 As is true in nature, no two breasts are identical. This is even more common with sagging breasts. After Breast Lift surgery, there is a period of healing and settling of the breasts. During this period breasts with different extent of sagging and laxity will settle at different rates. Therefore, it is very common to see some differences early on during the healing period. Afterwards, there may appear some slight differences between your breasts but it should be no more pronounced than that which would happen in breasts naturally. In some cases, additional surgery may be performed to improve symmetry.
As is true in nature, no two breasts are identical. This is even more common with sagging breasts. After Breast Lift surgery, there is a period of healing and settling of the breasts. During this period breasts with different extent of sagging and laxity will settle at different rates. Therefore, it is very common to see some differences early on during the healing period. Afterwards, there may appear some slight differences between your breasts but it should be no more pronounced than that which would happen in breasts naturally. In some cases, additional surgery may be performed to improve symmetry.
Fat Necrosis
There is a risk that small areas of fatty tissue deep within the breast might die. Sometimes, this causes hardness within that area of the breast that may be mistaken to be breast lumps. Mammogram can help differentiate between the two. In some cases, removal of fat necrosis through surgery may be necessary. Smokers have an increased risk of skin loss and wound healing.
Delayed Healing
Wound disruption or delayed wound healing is possible. Some areas of the breast skin or nipple region may not heal normally and may take longer to heal. This is especially common at the junction of the Inverted-T incision. Usually, these will heal without any sequel over several weeks.
Areas of skin or nipple tissue may die. This may require frequent dressing changes or further surgery to remove the non-healed tissue. Individuals who have decreased blood supply to breast tissue from past surgery or radiation therapy may be at increased risk for wound healing and poor surgical outcome. Smokers have a greater risk of skin loss and wound healing complications.
Sutures
Most surgical techniques use deep sutures. You may notice these sutures after your surgery. Sutures may spontaneously break through the skin, become visible or produce irritation that requires suture removal.
Nipple-Areola size and shape
Following Breast Lift the size, shape, and position of the nipples will not be identical as it is true in normal breasts. Depending on the skin elasticity of the two breasts one areola might stretch more than the other after a mastopexy.
As discussed earlier the peri-areolar mastopexy carries a higher incidence of stretching and enlargement of the areola, which might require further revision surgery.
Recurrent Ptosis
The breast skin and tissue continue to change with age, with gradual loss of its elasticity. Although Mastopexy can turn back the clock of aging, it cannot stop it. Those who have breasts with sun damaged thin skin and stretch marks, or those after weight loss, or with inherently poor elasticity are at a higher risk of developing recurrent ptosis early on. In this group there is also a relatively high incidence of “bottoming out” of the breasts. Under this circumstance the weight of the breast tissue can stretch out the lower breast skin causing the majority of the breast tissue slides below the level of the nipple, making it appear that the nipple is sitting too high on the breast.
Skin Discoloration/Swelling
Bruising and swelling normally occurs after a Breast Lift. The skin in or near the surgical site can appear either lighter or darker than the surrounding skin. It is very rare, however, for swelling and skin discoloration to be permanent.
Allergic Reactions
In rare cases, patients may experience allergies to tape, suture material and glues, blood products, topical preparations or injected agents. Sometimes these reactions also, rarely, include systemic reactions such as shock from drugs used during surgery and prescription medicines.
Anesthesia Reactions
All anesthesia, local or general, involves a risk of complications, injury and even death. You should interview your cosmetic surgeon thoroughly about the kind of anesthetist that he or she employs. While many surgeons use nurse anesthetists, the safest option is a physician who specializes in anesthesia. This is particularly true when the surgery is performed in a surgical facility other than a hospital. A physician anesthetist is better qualified to address any complications that may arise.
Future Pregnancy and Breast Feeding
It is possible that pregnancy will cause your breasts to enlarge and your breast skin to stretch and offset the mastopexy results.
As a general rule a Breast Lift or any breast surgery that involves rearrangement of the breast tissue can affect a woman’s ability to breast feed. Because during breast reduction the nipple is generally not detached or separated from the milk glands, there is a reasonable chance of preserving breast feeding ability.
Mastopexy Performed at the Time of Breast Implant Removal Surgery
Patients who opt for these procedures simultaneously may be at greater risk of skin necrosis (skin dying), and of the nipples and breast tissue due to decreased blood supply to the tissues from the implant removal.
Concerns with Results
The number one complaint after breast augmentation is that patients regret that they didn’t have larger implants. This arises from the fact that when trying on implants before surgery, women are either shy or have not gotten used to having larger breasts. To avoid this, I recommend that you choose the largest implant size that you can feel comfortable with.
The second most common reason for dissatisfaction after breast augmentation is that women feel that once they get breast implants they should instantaneously be ready for the swimsuit, with the “Perfect New Breasts”! Obviously, it takes weeks to months for implants to settle, swelling to subside, and breast tissue to accommodate the new implant. Therefore, be patient.
A third very common reason for dissatisfaction after breast augmentation is having unreasonable expectations. Most women quickly forget the shape of the breasts that they had before their augmentation, just several weeks ago. The esthetic outcome of Breast Augmentation greatly depends on what your breasts looked like before surgery. For example, if you had significant breast asymmetry, tubular breasts, or extensive sagging beforehand, surgery would not be able to give you “perfect breasts”, but only breasts that are better looking than where you started.
Seven steps to having a great result with your Breast Reduction?
- 1. Do your research.
- 2. Ask questions.
- 3. Check your doctor and surgery facility credentials.
- 4. Know your goal. What is it that you really want to achieve?
- 5. Have realistic expectations. No human can attain perfection!
- 6. Follow your doctor’s instructions thoroughly.
- 7. Be patient with getting there. You just had real surgery; and you didn’t buy breasts off the rack!